Welcome From the College President
I am thrilled that you are considering applying to Sentara College of Health Sciences. It’s hard to believe we’ve been here for more than 130 years! This institution consistently attracts the very best students in the region and helps transform them into extremely well trained and knowledgeable healthcare professionals.
What is most important to me is that all of our students graduate with a sense of professional self-esteem. We offer a flexible and supportive environment for every kind of student to reach that level of confident, professional capability. And through our uniquely accommodating programs, including distance education and hybrid learning, comprehensive hands-on training, and student support system, we can help you get there.
Students who excel in our programs are truly passionate about delivering quality healthcare. Many members of our faculty were previously students of the College who followed their passions to care for others at area hospitals before returning to us to share their excitement with you. Our students benefit from both our experienced faculty and our innovative teaching methods. This is an amazing place where your education can lead to a gratifying and successful career.
- Dr. Angela Taylor,
College President
Sentara College of Health Sciences
Approach to Education
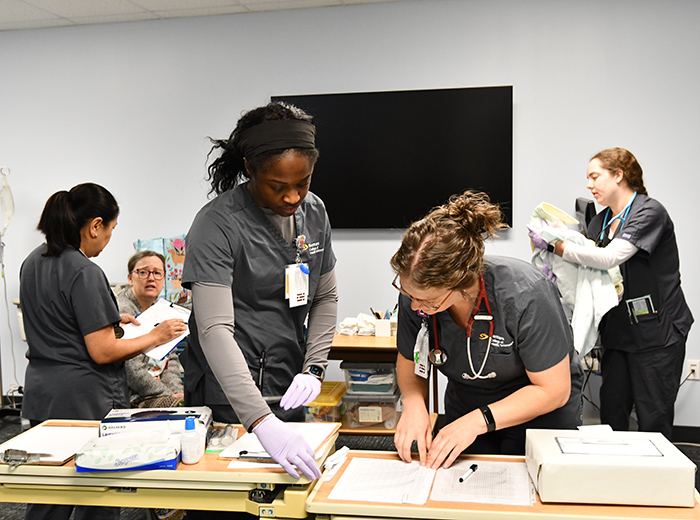
Envision working alongside fellow students as determined as you are to save a simulated patient’s life. Here, you’ll develop the skills and confidence necessary to step from the classroom into the real world. Through engaging classroom discussion and instruction to comprehensive, hands-on training in our simulation labs, you will learn how to use real skills to care for real patients. This practical understanding and application is what sets our graduates apart, and healthcare administrators locally and across the country know it.
Sentara College of Health Sciences is a thoroughly innovative institution that embraces a hybrid style of teaching and learning. Hybrid learning encourages students to take responsibility for their education through independent study online, while still engaging in traditional classroom discussions and hands-on clinical exercises. Through our online distance education classes, students have access to high-quality education and resources, with added flexibility for working professionals.
As a student, you will have access to Sentara Healthcare’s highly rated, state-of-the-art facilities, as well as doctors and mentors at the leading edge of their fields. Through our certificate programs, degree-granting programs, and hours of unmatched clinical experience, you will have the opportunity to build the professional experience that can support a long and successful career.